
Health
African countries paying Nigerian doctors three times higher – CMDs



He also said that countries like Sierra Leone and Gambia were offering them up to $3000 to $4000 which was about three to four times in the country.
Bassey, who is the CMD of the University of Uyo Teaching Hospital, said the health sector is currently undergoing a major crisis in terms of manpower as health professionals are leaving in droves.
He also said doctors often went on strike because the government often failed to meet unrealizable promises.
Bassey said this when he appeared before the House of Representatives Ad hoc Committee to probe employment racketeering in Federal Government agencies alongside the heads of other health institutions in the country.
He said, “Some African countries are also beginning to poach from Nigeria. The West Coast is looking for our specialists. So many people are now going to places like Sierra Leone and Gambia and the wages they earn are $3000 to $ 4000. It is about three to four times what they earn back home. So we are beginning to see that people are leaving for other African countries too.
“The health sector is currently undergoing a major crisis in terms of manpower. What we are seeing is that medical specialists, not just doctors, even nurses, in fact, even more nurses are leaving. Doctors, nurses, laboratory scientists, physiotherapists, radiographers, and all manner of health professionals are leaving the country in droves.
“That is part of the problem we are facing. Replacement of these health workers is a major problem. This is because even though we are usually granted approvals to recruit, getting the waivers is a tortuous process.”
He said due to the urgency of the need to replace various health professionals who leave, it is difficult to comply with federal character in recruitment.
He also noted that previous governments had reached ridiculous agreements because of their urgent need to end strike actions.
“ Now, they have agreements that they cannot implement. And then after a certain period, six months or one year and you have not implemented it, people now go on strike. So we need to sit down together and negotiate.”
The Chairman of the Ad hoc Committee, Hon Yusuf Gagdi, urged the doctors to be patriotic by staying back to contribute to the development of the country, even if they have better options abroad.
He said the committee would work towards addressing the need to balance compliance to the spirit of federal character and filling up urgent vacancies in the health sector.
Gagdi said, “I admit there is a lack of advanced medical facilities in our health sector. This is a fact and we must as governments pay attention to that. Where we are confused is the aspect of lack of patriotism.
“You ( Medical doctors) are produced by Nigerian institutions. We admit the brain drain and are trying to find solutions. We are happy to see you here. A lot of you have connections maybe based on the value of your intellect to be in the developed countries and provide services to them. But most of you find fashion in adding value to your own motherland and fatherland.
“What are you telling your co-professionals about patriotism, about giving back to the society that gave you the knowledge? We challenge you to be true to your own profession and the issue of morality. You cannot disown your father no matter how poor he is for taking you this far to go and adopt somebody’s father. Nigeria is our country.
“Nigeria produced us as medical doctors, no matter the rot within our public sector in terms of remuneration. Let us work together and see how we can find solutions to that. But let us remain in Nigeria to serve our own country.”
Gadgi added, “We would review your submissions entirely. For these institutions that have pending recruitment cases, we would interface with them uniquely. For those of you who don’t have one, we will look into your issue.
“You have a very good defense for now having a balanced sheet in terms of federal character. Nigerians have listened to you. So whatever this committee at the end of the day recommends to the government it is going to be done and it is for our own good entirely.”
In 2024, the Minister of Health and Social Welfare, Prof. Muhammad Pate, revealed that Nigeria had about 55,000 licensed doctors.
Speaking during an interview on Channels TV’s Politics Today, Pate disclosed that no fewer than 16,000 doctors had left the country in the past five years, while about 17,000 others had been transferred out of active service.
Worrisomely, a new revelation by the Lagos State Commissioner for Health, Prof. Akin Abayomi, indicates that the number of practising doctors in Nigeria has declined from 55,000 to 40,000 within just one year.
In his presentation at a one-day leadership dialogue in Lagos themed “Strengthening PHC Systems: A Joint Leadership Dialogue,” Abayomi identified manpower shortage as one of the most critical challenges facing the health sector.
The dialogue, organised by the Lagos State Primary Health Care Board with support from development partners, addressed barriers hindering PHCs from meeting expectations and proposed practical solutions for building sustainable PHCs with lasting impact.
Abayomi stated that Lagos currently has only 7,000 doctors serving an estimated 30 million residents, far below the number needed for optimal care delivery.
The commissioner raised concerns over the acute shortage of health workers in the state, disclosing that the state requires an additional 33,000 doctors to meet the healthcare demands of its growing population.
“Nigeria currently has about 40,000 doctors against an estimated need of 300,000, while Lagos alone requires about 33,000 doctors but has only about 7,000,” he said.
According to him, Lagos’ doctor-to-population ratio remains far below what is required for optimal healthcare delivery, noting that the state’s doctors are serving an estimated population of nearly 30 million people.
To address the shortfall, Abayomi said the state government is investing in its newly established University of Medicine and Health.
“Within five years, UMH will produce about 2,500 healthcare workers annually, including laboratory scientists and other essential cadres,” he stated.
The mass exodus of healthcare professionals popularly known as japa syndrome, especially doctors, nurses, and pharmacists has remained a major concern in Nigeria.
A 2017 survey conducted by a Nigerian polling organisation in partnership with Nigeria Health Watch revealed that about 88 per cent of Nigerian doctors were seeking job opportunities abroad at the time.
The President of the Nigerian Medical Association, Prof. Bala Audu, recently warned that Nigeria has moved beyond passive brain drain and has become a direct recruitment hub for foreign governments seeking skilled medical professionals.
In an interview, Audu revealed that international recruiters now visit Nigeria to directly hire doctors—particularly specialists such as obstetricians, gynaecologists, and paediatricians—offering them superior working conditions, remuneration, and infrastructure.
He lamented that while Nigeria’s population continues to grow and mortality rates remain high, the country is losing specialists at an alarming rate.
“Many of our doctors are not even going abroad to look for jobs. Foreign governments now come into Nigeria to pick doctors and take them away,” Audu said.
“We are still having more births, yet maternal deaths remain high because the skilled birth attendants who should care for these women are reducing every day.”
Audu added that in some specialties, the number of Nigerian doctors practising abroad may already exceed those still working within the country, a situation worsened by the government’s failure to significantly improve doctors’ welfare despite existing policy frameworks.
Experts have warned that with the current pace of emigration, it would be impossible for Nigeria to produce enough health workers to meet its growing healthcare demands. They estimate that it would take at least 20 years to train the over 400,000 health workers required to close the gap.
A former President of the NMA, Prof. Mike Ogirima, described Nigeria’s doctor-to-patient ratio as “horrible,” noting that the country currently has about one doctor to 8,000 patients—far below the World Health Organisation’s recommendation of one doctor to 600 patients.


Nigerian health communication researcher, Ifesinachi Ayogu, has attributed the rising number of cancer-related deaths in the country to the neglect of routine self-breast examination among women and routine Prostate-Specific Antigen (PSA) testing among men.
Ayogu told journalists on Monday that the failure to prioritise regular screening had contributed significantly to late detection of breast and prostate cancers, which are among the leading causes of cancer-related deaths in Nigeria.
He said many cancer cases were only discovered when the disease had reached advanced stages, making treatment more complex and survival chances lower.
According to him, the increasing burden of cancer deaths calls for a more intentional and sustained approach to cancer awareness, early detection, and preventive health behaviour.
“Early detection saves lives, but many people are not practising simple, routine screening that could help detect cancer early,” Ayogu said.
He noted that breast cancer and prostate cancer were often manageable when detected early, but ignorance, fear, stigma, and limited awareness continued to discourage people from carrying out regular checks.
The researcher explained that self-breast examination allows women to notice unusual lumps or changes early, while routine PSA testing helps detect prostate abnormalities before symptoms become severe.
Ayogu said deaths resulting from breast and prostate cancers were often preventable, stressing that delayed diagnosis was a major factor contributing to high mortality rates.
He added that many Nigerians still lacked basic information on how to conduct self-breast examinations, when to go for PSA tests, and where to seek appropriate medical care.
The health communication researcher emphasised the need for community-based education, especially in rural areas, using trusted platforms such as churches, markets, women’s groups, and radio programmes to promote routine screening practices.
He also urged healthcare providers and public health institutions to intensify public education on cancer prevention and ensure that screening information was simple, accurate, and accessible.
Ayogu advised individuals with a family history of breast or prostate cancer to be particularly vigilant about routine screening and healthy lifestyle practices.
He stressed that promoting routine self-breast examination and PSA testing would play a critical role in reducing late presentation and improving cancer survival outcomes in Nigeria.
Ifeshinachi Ayogu is a PhD graduate student, at the University of Oklahoma United States of America, his core interest is cancer communication, according to him, he believes that the next breakthroughs in cancer care for Nigerian women and men will not come from medicine alone.


The Federal Government said it had intensified monitoring and screening procedures at all points of entry in response to the ongoing outbreak of the Ebola Virus Disease in the Democratic Republic of Congo.
The Director of Port Health Services at the Federal Ministry of Health and Social Welfare, Dr Akpan Nse, disclosed this in an exclusive interview with Saturday PUNCH on Friday.
Nse also noted that additional staff had been employed to strengthen border surveillance in the country.
Health authorities in the Democratic Republic of Congo declared an outbreak of Ebola virus disease in Kasai Province, where 28 suspected cases and 16 deaths, including four health workers, had been reported as of September 5, 2025.
The outbreak comes at a time when much of Central and West Africa is grappling with overlapping health and humanitarian crises, including cholera, malnutrition, and population displacement.
The DRC’s last outbreak of Ebola virus disease occurred in the north-western Equateur Province in April 2022.
It was brought under control within three months.
In Kasai Province, previous Ebola outbreaks were reported in 2007 and 2008. Overall, the country has experienced 15 outbreaks since the disease was first identified in 1976.
Ebola virus disease is a rare but severe, often fatal illness in humans.
It is transmitted to people through close contact with the blood, secretions, organs, or other bodily fluids of infected animals such as fruit bats (believed to be the natural hosts). Human-to-human transmission occurs through direct contact with the blood or bodily fluids of an infected person, contaminated objects, or the body of someone who died from the disease.
In the ongoing outbreak, samples tested on September 3 at the National Institute of Biomedical Research in the capital, Kinshasa, confirmed that the cause was Ebola Zaire, a strain of the Ebola virus.
Dr Nse noted that although Nigeria was at risk of importing the virus due to high levels of international travel with the DRC, Port Health Services was on alert and had strengthened surveillance to prevent this.
He said, “We have intensified surveillance at all points of entry across the country—airports, land borders, and seaports. Every inbound traveller coming from Congo to Nigeria is thoroughly screened, and we collect their medical history through mandatory forms.
“We have also reactivated our portals. Every passenger on every flight coming to Nigeria from Congo is screened upon arrival. This applies to airports, seaports, and land borders. Even if passengers transit through Congo on their way to Nigeria, they must undergo screening.
“In addition, with support from WHO, we have recruited more staff to enhance surveillance. Increasing the workforce allows us to effectively prevent the importation of the virus and ensure thorough screening at all borders.”
He added that some private organisations had partnered the Federal Government to ensure that thermal scanners at airports remained fully functional.
Meanwhile, the WHO has released $500,000 from its Contingency Fund for Emergencies to support the response to the Ebola Virus Disease outbreak in the DR Congo.
Announcing this at a media briefing on global health issues on Friday, the WHO Director-General, Dr Tedros Adhanom Ghebreyesus, disclosed that 28 suspected cases and 16 deaths had been reported so far, including four health workers.
He highlighted that the UN body already had staff on the ground in Kasai, with more on the way.
“We’re joining rapid response teams to trace contacts and find cases; we’re collecting and testing samples, and we’re providing technical expertise in surveillance, infection prevention and control, treatment, risk communication, and more. WHO has also delivered personal protective equipment, laboratory equipment, medical supplies, and a mobile laboratory.
“We had previously prepositioned 2000 doses of Ebola vaccine in Kinshasa, which we are releasing to vaccinate contacts and health workers. This is the 16th outbreak of Ebola in the DRC, and the government has rich experience from those previous outbreaks,” the WHO boss stated.


“Go and Verify”: How Sunday Umeha Is Redefining Representation in Ezeagu/Udi
Chief Sir Paul Chukwuma Lays His Beloved Sister to Rest


2027: Anambra ADC Intact Despite Obi, Kwankwaso Departure – Guber Candidate






-
 News5 years ago
News5 years agoUncompleted structures in Enugu to undergo integrity test – Authority
-
 News4 years ago
News4 years agoBREAKING: FG to release Nnamdi Kanu tomorrow, fixes emergency hearing
-
 News2 years ago
News2 years agoBREAKING: Former Anambra Governor is Dead
-
 Entertainment4 years ago
Entertainment4 years agoChrisland School Girl’s Online Activities Leak [Video]
-
 Social event4 years ago
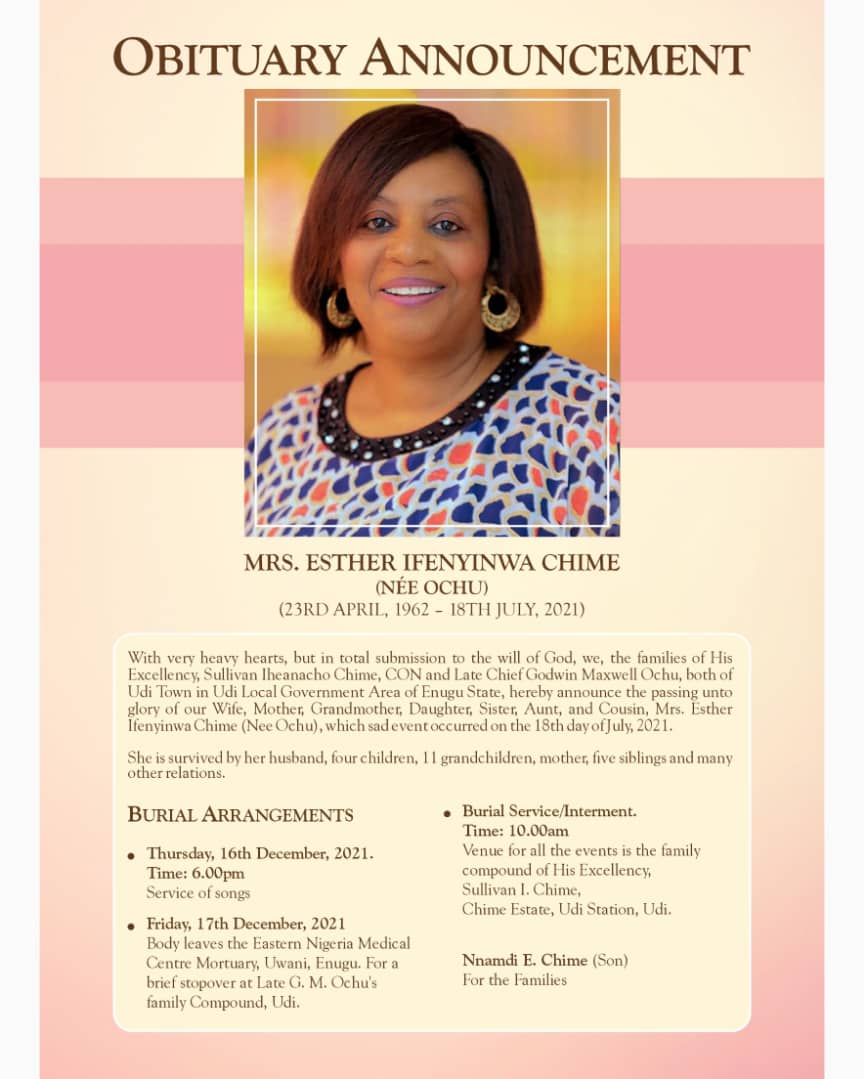
Social event4 years agoEx-Enugu governor, Sullivan buries wife December 17
-
 Politics2 years ago
Politics2 years agoEnugu spends the least as 30 govs burn N968.64bn on refreshments, others in 3 months
-
 Foreign2 years ago
Foreign2 years agoDenmark announces visas for, welders mechanics, bricklayers, others
-
 Crime5 years ago
Crime5 years agoBREAKING! Sit-at-home: Vehicle conveying tomatoes, set ablaze in Enugu












